Introduction
Victim identification using hard tissue evidence from skeletal and dental tissue remains an important tool in forensic identification. These evidentiary materials unlike soft tissue landmarks are more stable and can provide valuable information by observational analysis and radiographic assessment of antemortem and postmortem data.[1],[2] Similarly, soft tissue parameters like digital ridge patterns are indicative of genetic variations among different population pools and can aid as important anthropological parameters in establishing racial placement and genetic linkage.
Defects in embryological developmental milestones are evident as postnatal deviations from normal human anatomical structure. Craniofacial developmental anamolies have been extensively studied in the past either as population characteristics or as isolated genetic defects. Most common craniofacial developmental anomalies include skeletal and dental malocclusions.[2],[3] The digital ridge patterns are indicators of growth-related developmental patterns. These patterns start to appear during 12th week of intrauterine life. Their development completes by 24th week after which they persist throughout life.[3] Study of ridge patterns is known as ‘Dermatoglyphics’. Cummins and Midlo (1926) defined ‘dermatoglyphics’ as the study of patterned traceries of fine ridges on digits, palms and soles. Abnormal dermatoglyphics patterns have been observed in conditions like Down’s syndrome, Turner’s syndrome, Klinefelter’s syndrome, leukemia and thalidomide exposure.[4] Digital ridge patterns were first classified by Sir Francis Galton (1892) into- arches, loops and whorls.[5] These patterns are formed around the same time as the craniofacial skeletal and dental growth. Hence, it is necessary to determine any probability of correlation between dental (Angle’s classification) and skeletal (ANB) malocclusions and digital ridge patterns in the North Indian population subset analyzed in this study. The null hypothesis of this study was that there is an existence of correlations among dental and skeletal malocclusions and digital ridge patterns. Both of these parameters can have geographic and racial bearings, since the genetic profiles of different populations vary in expressivity. Hence, their phenotypes exhibit genetic variability pertaining to geographical differences and various racial profiles.
Methods
This pilot study cohort comprised of 60 subjects (44 females and 16 males) age ranging between 18 to 23 years who reported for orthodontic correction. Subject selection criteria included- presence of permanent dentition and the absence of any systemic conditions affecting musculoskeletal system. Informed written consent was obtained from participants as per guidelines of Declaration of Helsinki. Lateral cephalogram radiographs were studied using Steiner’s analysis for skeletal malocclusion (ANB angle) (Figure 1). Dental malocclusion was assessed using Angle’s classification. Digital imprints were obtained using an ink stamp pad and plain paper. Finger print patterns observed were identified as- loop, plain arch, tented arch, whorl, outer whorl and meet whorl patterns (Figure 2). The ridge patterns were analyzed and correlated with corresponding dental and skeletal malocclusion.
 | Figure 1 : Tracing Photograph Of Skeletal Class Ii Malocclusion.
 |
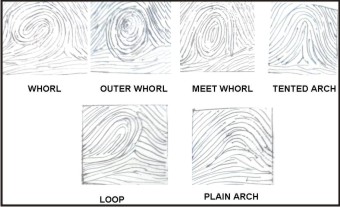 | Figure 2 : Digital Ridge Patterns Evaluated In The Study.
|
For correlative purposes, groups were formed as: Group 1: Skeletal and dental malocclusions; Group 2: Females and dental malocclusion; Group 3: Males and dental malocclusion; Group 4: Females and skeletal malocclusion; Group 5: Males and skeletal malocclusion; Group 6: Females and ridge pattern; Group 7: Males and ridge patterns; Group 8: Class I dental occlusion and ridge patterns; Group 9: Class II dental malocclusion and ridge patterns; Group 10: Class III dental malocclusion and ridge patterns; Group 11: Class I skeletal (2±2°) malocclusion and ridge patterns; Group 12: Class II skeletal (>4°) malocclusion and ridge patterns; Group 13: Class III skeletal (<2°) malocclusion and ridge patterns; Group 14: Combined Class I and Class II dental malocclusions and ridge patterns; Group 15: Combined Angle Class II and III malocclusions and ridge patterns; Group 16: Combined Angle Class I and III malocclusion and ridge patterns.
One way Analysis of Variance (ANOVA) and Tukey-Kramer multiple comparison tests were employed for ascertaining P value.
Results
Statistical observations indicated that a significant relationship (P=0.04) exists between dental and skeletal malocclusions (Table 1). Extremely significant correlations (P<0.0001) were observed between gender and skeletal and dental malocclusions (Tables 2 and 3). No significant relationship was observed between Class I/III dental malocclusions and ridge patterns (Table 4). On the other hand, a significant correlation (P=0.02) was observed between Class II dental malocclusion and ridge pattern (Table 4). Similarly, no correlation was observed between Class I/III skeletal malocclusions and ridge patterns (Table 5). Class II skeletal malocclusion and ridge patterns exhibited extremely significant (P<0.0001) correlation (Table 5). Sexual dimorphism had a significant correlation with ridge patterns (Table 6). No correlations were observed in groups 14, 15 and 16 (P=0.98, 0.99, 0.99, respectively) (Table 4).
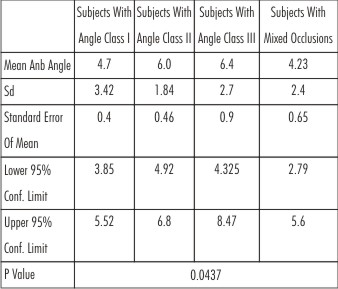 | Table 1 : Table Showing Statistical Relationship Between Dental And Skeletal Malocclusions
|
 | Table 2 : Table Showing Relationship Between Gender And Dental Malocclusion
|
 | Table 3 : Table Showing Relationship Between Gender And Skeletal Malocclusion (Anb Angle)
|
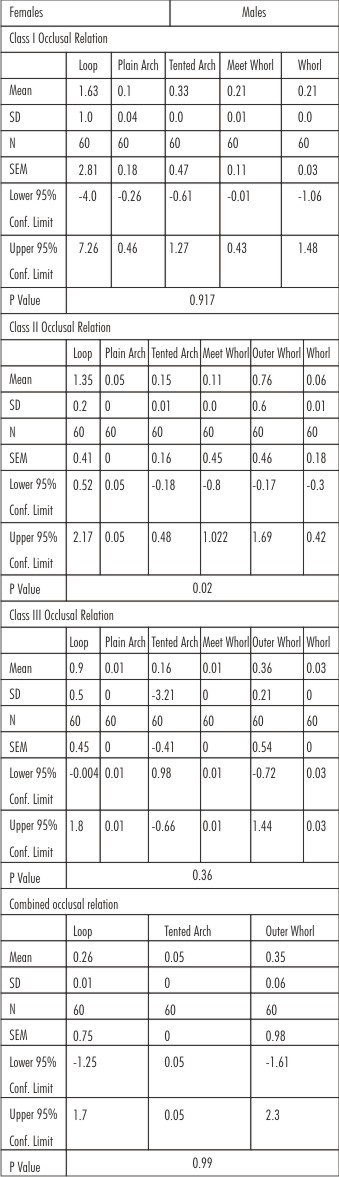 | Table 4 : Table Showing Association Between Digital Ridge Patterns And Dental Malocclusion
|
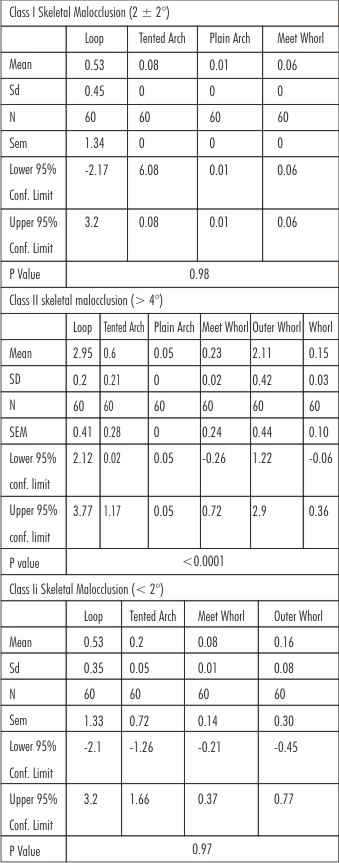 | Table 5 : Table Showing Relationship Between Skeletal Malocclusion And Ridge Patterns
|
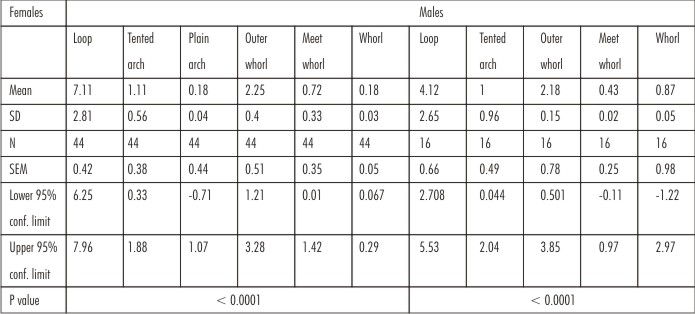 | Table 6 : Table Showing Relationship Between Gender And Ridge Patterns
|
Discussion
Alterations in embryological development influence the craniofacial structures, dental development and other bodily parameters such as appendage features like digital ridge patterns. These manifest as malocclusions and variations in dermatoglyphics patterns that might have demographical and racial differences. This study analyzed correlations between skeletal and dental malocclusions and dermatoglyphics patterns that have strong genetic association. Sexual dimorphism exhibited extremely significant inter-relationship with skeletal and dental malocclusions. De Freitas et al (2005) reported no statistically significant difference between Class II division1 skeletal malocclusion and genders.[6] Strong genetic association was observed between genders and dermatoglyphic patterns in this study. A positive association was observed between skeletal Class II and Angle’s Class II dental malocclusions and ridge patterns. Sidlauska et al (2006) also observed that Class II div 1 malocclusion is the most common skeletal malocclusion.[7] This study is in contradiction to Reddy et al (1997) who reported no correlation between dermatoglyphic patterns and various dental parameters.[8] Mridula et al (2001) also reported negative correlation between ridge patterns and dental malocclusion.[3] Osunwake et al (2008) studied ethnic Nigerian population and observed no statistical significant relation between Class II division I skeletal malocclusion and genders.[5] Bacetti et al (2005) observed a significant degree of association between Class III dental malocclusion and sexual dimorphism. No such relation was observed in this study.[9] Current study provided essential and important information regarding malocclusions of dental and skeletal variety and digital ridge patterns which was unique to the population subset studied i.e., significant correlation was observed between Class II skeletal and Angle’s Class II malocclusions with digital finger print patterns. Hence, it can be concluded that genetic differences exist among various population subsets which are reflected in developmental growth patterns manifesting in neural crest derived structures. These findings provide a baseline framework reference for anthropological analysis for comparison of phenotypic variations among different genetic pools and hence, act as important personnel identification forensic tool.
References
1. Ryan E.J. Identification through dental records. J Crim Law and Criminol 1937;28(2):253-60.
2. Okusa N, Nishio H, Noda H, Tatsumi S. A case study in estimating age based on forensic odontological findings in skeletal remains. Acta Med Kinki Univ 2011;36(1):37-40.
3. Trehan M, Kapoor DN, Tandon P, Sharma VP. A correlative study of dermatoglyphic pattern with malocclusion. J Ind Orthod Soc 2001;34:114-125.
4. Ghodsi Z, Shahri NM, Ahmadi SK. Quantitaive and qualitative study of dermatoglyphic patterns in albinism. Curr Res J Biol Sci 2012;4(4):385-388.
5. Osunwake EA, Ordu KS, Hart J, Esomonu C, Tamunokuro FB. A study on the dermatoglyphic patterns of Okrika and Ikwere ethnic groups of Nigeria. Scient Afr 2008;7(2):143-147.
6. de Freitas MR, dos Santos MAC, de Freitas KMS, Janson G, de Freitas DS, Henriques JFC. Cephalometric characterization of skeletal Class II division 1 malocclusion in white Brazilian subjects. J Appl Oral Sci 2005;13(2):198-203.
7. Sidlauska A, Svalkauskiene V, Sidlaukas M. Assessment of skeletal and dental pattern of class II division 1 malocclusion with relevance to clinical practice. Stomatologia Batic Dent Maxillofac J 2006;8:3-8.
8. Reddy S, Prabhakar AR, Reddy VVS. A dermatoglyphic predictive and comparative study of Class I, Class II div 1 and Class III malocclusions. J Ind Soc Pedo Prev Dent 1997, 13-19.
9. Baccetti T, Reyes BC, McNamara JA. Gender differences in Class III dental malocclusion. Angle Orthod 2005;75:510-520.
|